This is not to say that this is entirely correct but it is something that we do have to think about. What if coronavirus, Covid-19, is really just the old man’s friend in a new guise?
It being necessary to be more than a little blunt here. The process of dying is not a happy nor, often enough, swift one. So much so that pneumonia used to be known as “the old man’s friend”. One or other of the more disgusting diseases to which humans are prey was eating away at the near senescent. Or even, senescence had taken hold but little was physically wrong. And then along came a viral infection which took the old lad away. Over the course of a couple of days. Allowing the deathbed scene with the massed generations of the family seeing granpops wheeze his last and then there were ham sandwiches.
We are all going to go and there’s a certain relief at going that way rather than, say, screaming into the night from the agonies of an advanced cancer. Or liver failure, a horrible way to go as those idiots who try overdosing on paracetamol rapidly find out.
No, this is not a paean of praise for the euthanasia of the aged. It’s just an observation of what our ancestors used to think.
The flip side of this was that pneumonia was – is – something that preferentially takes the old. As with influenza. The young and fit tend to be able to fight it off – and sure, we’ve drugs and treatments to help in doing so – and yet even so thousands do die of such each and every year and for most who do it’s the existence of some other problem that makes the addition the killer. The life so cruelly cut short would have been measured in weeks or months anyway.
One of our readers – herself a retired doctor and, as it happens, survivor of pneumonia – points us to this:
Roma, 13 mar 19:12 – (Agenzia Nova) – Le persone morte a causa del coronavirus in Italia, che non presentavano altre patologie, potrebbero essere solo due. E’ quanto risulta dalle cartelle cliniche finora esaminate dall’Istituto superiore di sanità, secondo quanto riferito dal presidente dell’Istituto, Silvio Brusaferro, nel corso della conferenza stampa tenuta oggi presso la Protezione civile a Roma. “I pazienti deceduti positivi hanno una media di oltre 80 anni – 80,3 per l’esattezza – e sostanzialmente sono prevalentemente maschi”, ha detto Brusaferro. “Le donne sono il 25,8 per cento. L’età media dei deceduti è significativamente più alta rispetto agli altri positivi. Le fasce d’età superiori ai 70 anni, con un picco tra gli 80 e gli 89 anni. La maggioranza di queste persone è portatrice di patologie croniche. Soltanto due persone non sono risultate al momento portatrici di patologie”, ma anche in questi due casi, l’esame delle cartelle non è concluso e potrebbero, dunque emergere cause di morte diverse dal Covid-19. Il presidente dell’Iss ha precisato che finora dagli ospedali di tutta Italia sono pervenute “poco più di cento cartelle cliniche”.
Ah, no, that’s not going to work as not all here are multilingual. So, as well as machines can do this these days:
Rome, 13 Mar 19:12 – (Agenzia Nova) – There may be only two people who died from coronavirus in Italy, who did not present other pathologies. This is what emerges from the medical records examined so far by the Higher Institute of Health, according to what was reported by the President of the Institute, Silvio Brusaferro, during the press conference held today at the Civil Protection in Rome. “Positive deceased patients have an average of over 80 years – 80.3 to be exact – and are essentially predominantly male,” said Brusaferro. “Women are 25.8 percent. The average age of the deceased is significantly higher than the other positive ones. The age groups over 70 years, with a peak between 80 and 89 years. The majority of these people are carriers of chronic diseases. Only two people were not presently carriers of diseases “, but even in these two cases, the examination of the files is not concluded and therefore, causes of death different from Covid-19 could emerge. The president of the ISS has specified that “little more than a hundred medical records” have so far come from hospitals throughout Italy.
These are the first minimum detailed data provided so far by the Civil Protection on the causes of death of coronavirus patients. At present, in fact, the authorities are unable to distinguish those who died from the virus, from those who, on the other hand, are communicated daily to the public, but who were mostly carriers of other serious diseases and who, therefore, would not have died from Covid-19. In response to a question from “Agenzia Nova”, in fact, Brusaferro was unable to indicate the exact number of coronavirus deaths. However, the professor clarified that, according to the data analyzed, the vast majority of the victims “had serious pathologies and in some cases the onset of an infection of the respiratory tract can lead more easily to death. To clarify this point , and provide real data, “as we acquire the folders we will go further. However, the populations most at risk are fragile, carriers of multiple diseases “.
This is getting very close to identifying the coronavirus as being just another seasonal ‘flu, the usual culling of the aged of the herd through pneumonia.
And for this we are closing down civilisation?
Again, we do not say this is absolutely true. We do though insist that it’s a view that has to be considered.
Charles McKay did point out, back in 1841, that we humans are prey to Extraordinary Popular Delusions and the Madness of Crowds.
We can add more recent examples. That American property values would only ever go upwards. That Simon Cowell has a use. That government is capable of running an economy and so on.
The point being that it really is possible for society to fall into the grip of some mania. That society is still here means we do wake up at some point but the earlier the better perhaps. Pet rocks lasted a few months and did no real harm. That government knows best idea is still skinning the people of Venezuela years after it was proven to have failed.
At which point we do come to that rather brutal calculus. If this is acting like pneumonia does, this coronavirus, then we’re going about dealing with it in entirely the wrong way. Note, again, the “if” there.
To give some numbers. And recall that our management task, however we achieve it, is the greatest flourishing of human beings that can be managed. Not quite Benthamism, the greatest good of the greatest number, for that always does come with the self-appointed Bentham assuming that heavy burden of deciding what is best for everyone. We also do not mean mere money, we are talking about utility, that thing that each and every one of us gets to decide for ourselves.
So, how to we apportion NHS money? A treatment that costs more than £30,000 per year of decent life saved (Qualy) doesn’t get funded. OK, £50,000 if people really argue about it – meaning if it’s politically fashionable this year, this disease.
Note the importance of the measure here – it is years of decent life saved that matter. Saving someone from pneumonia does indeed provide decent years of life. It’s something that is recovered from. The incidence of the treatment happens and there we are, life carries on until whatever else it is brings it to an end. But the implication of that calculus is that spending decent sums on keeping Granny going for a few weeks doesn’t pass the test – or at some price doesn’t – while Little Jimmy, aged four and a half and expecting to be seeing in the next millennium does justify that same treatment at that same expense.
How many years of life after treatment is not just important it’s the very essence of the decision.
To some numbers. One recent guess at the economic cost of Covid-19 is 14% of GDP for a quarter. For the UK that’s 2 trillion times 14%, or £280 billion. That’s not the cost of treating people, of course, it’s the loss we’re making by trying to avoid having to treat people. In order for this to make sense we need to be saving 5.6 million man years of life by making that loss.
Yes, yes, loss of GDP isn’t the same as resources spent on medical treatment and all that but this is still how we need to be doing the calculation. You can insert whatever numbers you prefer, the logic is still the same.
To get slightly better numbers we should divide by four – that quarter – and say 1.4 million man years of life. If we give 140,000 people another 10 years of life, or 35,000 another 40 years, our – admittedly crude – calculation says this is worth it. But if it’s a few tens of thousands living another few months then we’re grossly overdoing the reaction, aren’t we?
At some point we should – for the maximisation of human utility, not for something so base or crass as mere money – say the hell with it and allow the disease to rip through society. That this is true is obvious – there is some point at which this is true.
Charles McKay made the point that often enough a society will go beyond that point. The issue for us to consider is whether we’ve already done so. The uncomfortable answer being that we might well have done.
Addendum. A working out of those life year costs:
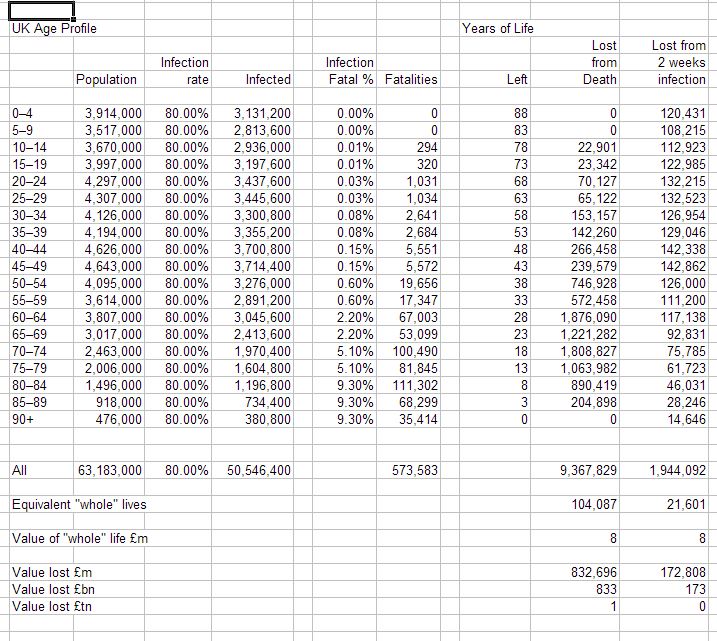
Note this assumes an 80% infection rate across the population. Plus the worst mortality rates we’ve seen – which we are really rather sure are wrong given unidentified infections.



{kind=link}
My take, with the hindsight from Italy, South Korea, and the Diamond Princess, is as follows:- Where hospital treatment is available for all serious cases then only the old and sick die, albeit many relatively young and fit require treatment. Presumably the treatment is necessary for the survival of the young and fit. There being a finite amount of treatment available the fear was that there would be insufficient to keep the young and fit alive. Given that treatment is becoming more efficient (it’s amazing what can be learnt once people have a reason to apply themselves) that problem is… Read more »
I’m not sure many, if any, young and fit require hospitalisation? Certainly very few require an ICU bed, which is the real capacity issue.
From Chinese data, 0.2% of under 25’s require hospitalisation, with 0.01% fatality rate. That INCLUDES those already in poor health. (UK 0.5% of U18 are in poor health).
We should reopen the schools and instead concentrate on ring fencing older and at risk people. We could get through the whole thing in 6-8 weeks and go back to normal.
I find it absurd that people are suggesting draconian measures for 65 million people, that wreck our economy, rather than draconian measures for the 3-4 million actually at risk. We can identify easily people who are pensioners and we can institute pretty good care for them at a tiny fraction of the cost of other measures. Keep the elderly in quarantine for six to eight weeks and we are probably pretty much all right by then.
As the majority of the at-risk elderly are retired, there is not much loss to economy if they just stay out of harm’s way for a bit. It doesn’t even require quarantine, just a little less socialising.
On Diamond Princess a high proportion of 20-50 year olds received medical attention. None of them died. It is of course unknowable how many would have survived anyway, but presumably the treatment did improve their chances. I wouldn’t trust the Chinese government to tell me the spelling of their leader’s name. Two months ago they were still maintaining that the disease didn’t transmit between humans. It should be remembered that the government’s rationale for banning sporting events was initially to free up the medical staff that would otherwise attend. BTW ignore the reported number of cases, at least until it… Read more »
But what was “medical attention”? Taking their temperature and handing out some paracetamol? I don’t believe any were the equivalent of hospitalised. And yes, as in my other comment, I’ve build a simple model that replicates an infection growing quickly based solely on increasing non-randomised testing of a decreasing number of infected people. I have a dim recollection of being told about that years ago, possibly at university. I am very suspicious that the “epidemic” is at least party a function of increased testing of a population that already has a large number of infections.
I think the reasoning is sound and Pat is right about the medical rationing of treatment. The non-economic problem is that the medical staff involved are stressed by having to make these decisions.. OK. modern humans are not as emotionally tough as their ancestors who lost up to half or more of their children and healthy grandparents were not common. Given the idiotic panic buying I am seeing and the occasionally simple rational responses in some country towns, (take a bow, Wangaratta) I fear the sales slump for supermarkets in two months as the massive stashes of non-perishables becomes a… Read more »
A question I posed yesterday on Twitter. Is CV, by itself, actually fatal to anyone? Are we seeing what look like clusters because there are in fact clusters of other diseases, such as flu? This morning, having recalled something I was taught years ago, I built a simple Excel model that produced a typical infection graph based on nothing more than daily increasing non-random testing. It is possible to show an epidemic with the model even as total actual infections decreases, provided the starting number of infections was sufficiently larger than the number of tests being done. I’m not saying… Read more »
My reading is that COVID by itself could well be fatal to anyone if left untreated, but not to anyone receiving treatment.
Otherwise it only finishes off those already in a poor way.
It’s difficult to know, but it does seem to be true that you need to at least be old to require hospital treatment to survive. But that is true for a large number of diseases, including flu each winter.